The Jaffe and enzymatic methods are the two most common methods for measuring serum creatinine. The Jaffe method is less expensive than the enzymatic assay ($0.30 vs $2.00 per test based on 2014 list prices) but is more susceptible to interferences. Although these tests are not expensive, they are high-volume tests and the savings could be substantial. We were using the enzymatic assay at the University of Utah and estimated that we could save about $50,000 per year by switching to the Jaffe assay; however, we were uncertain whether the Jaffe assay was safe to use due to the potential for interferences. For that reason, we decided to conduct a risk assessment to evaluate the suitability of the Jaffe assay.
Risk is defined as the expected cost of an action. The expected cost has two components: 1) the probability that an event will occur and 2) the consequences or cost of an event:
Risk = prob(event) x cost(event)
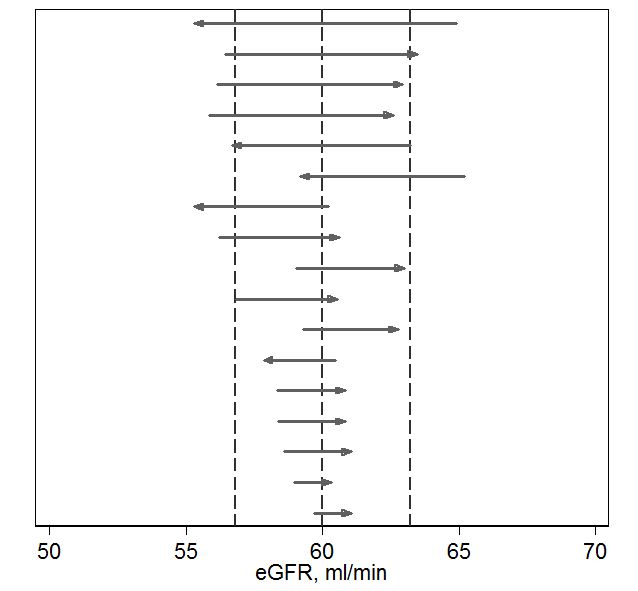
The event of interest was misclassification of a patient due to an error in serum creatinine measurement. Nephrologists classify kidney disease based on the estimated glomerular filtration rate which is based on the creatinine value. The distribution of eGFR for patients at our hospital is shown in Figure 1. The dashed lines show decision limits that nephrologists use to classify kidney disease. An eGFR is considered normal or healthy.
We spoke with the nephrologists and learned that they were relatively unconcerned about errors in eGFR in healthy patients (eGFR above 60 ml/min) because there was no potential for harm. Similarly, they felt there was relatively little risk of harm to patients with low eGFRs because these patients are routinely monitored and no major decision would be based solely on a single eGFR measurement. An error in creatinine measurement in a low eGFR patient would be detected by repeat measurements or be inconsistent with other measurements. From the nephrologists’ point of view, the only area of concern was in the region around 60 ml/min. Patients about 60 ml/min are considered healthy whereas those below 60 ml/min are diagnosed with stage 3a chronic kidney disease. In this zone, an error in serum creatinine could result in a false negative (i.e. observed eGFR greater than 60 ml/min when the true eGFR was less than 60 ml/min). In such cases, a patient may go without care and their disease could progress. The nephrologists believed that the potential for harm was relatively minor, but potential for harm did exist.
We compared the eGFRs provided by the enzymatic and Jaffee methods to estimate how often patients might be misclassified (Figure 2).1 Focusing on the 60 ml/min decision limit, we found that 17 of 500 (3.4%) of measurements were discordant. Some of these discordant results would be due to imprecision. Discordance due to imprecision would have small differences (bottom of Figure 2) and are unavoidable – they would occur using any method. Discordance due to interference would be expected to have larger differences (top of Figure 2) and could be avoided by using the enzymatic method. We used statistical techniques to estimate the proportion of discordances that were due to interference vs imprecision and found that about 60% of the discordance at the 60 ml/min limit was due to interference. In summary, our risk analysis showed that using the Jaffe method would pose about a 2% rate of avoidable misclassification which presented some potential risk to patients. The nephrologists felt the risk was low but, in theory, disease could unnecessarily progress in a patient with a false negative diagnosis.
Our risk analysis was based on analytical error. We compared magnitude of analytical error to the biological variation in eGFR and found that the analytical error was relatively small in comparison to biological variation (data not shown). Biological variation was likely to be a more significant cause of misclassification than analytical error.
So, what to do? Was the potential savings of the Jaffe method worth the risk? Some experts recommend against using the Jaffe method. 2-4 On the other hand, most US laboratories use the Jaffe assay. A recent College of American Pathologists proficiency challenge found that 70% of the submitted results were based on the creatinine assay.5
We decided to get the best of both worlds by using BOTH methods. We defined a zone of risk surrounding the 60 ml/min eGFR decision limit (Figure 3). Results in this zone would have some risk of misclassification whereas results outside of the zone would be unlikely to be misclassified using the Jaffee method. All creatinine measurements are initially performed using the Jaffe method. If the result is outside the risk zone, the result is reported. If results fell within the risk zone, they were repeated with the enzymatic method and the results of the enzymatic method are reported. This reflex procedure saves money while avoiding risk. The reflex rate is approximately 15%.
There are circumstances in which one would want to order the best possible test. To that end, we created a special orderable test, based on the enzymatic method, that the nephrologists could use to insure the most accurate results when required. For example, the enzymatic test may be indicated when making decisions regarding biopsies for renal transplant patients. The order volume for the special test has been less than 100 orders per year.


References
- Schmidt RL, Straseski JA, Raphael KL, Adams AH, Lehman CM. A Risk Assessment of the Jaffe vs Enzymatic Method for Creatinine Measurement in an Outpatient Population. PloS one. 2015;10(11):e0143205.
- Cobbaert CM, Baadenhuijsen H, Weykamp CW. Prime time for enzymatic creatinine methods in pediatrics. Clinical Chemistry. 2009;55(3):549-558.
- Drion I, Cobbaert C, Groenier KH, et al. Clinical evaluation of analytical variations in serum creatinine measurements: Why laboratories should abandon Jaffe techniques. BMC Nephrology. 2012;13(1).
- Panteghini M. Enzymatic assays for creatinine: time for action. Scand J Clin Lab Invest Suppl. 2008;241:84-88.
- College of American Pathologists. Chemistry/Therapeutic Monitoring, Participant Survey. 2014.

-Robert Schmidt, MD, PhD, MBA, MS is currently an Associate Professor at the University of Utah where he is Medical Director of the clinical laboratory at the Huntsman Cancer Institute and Director of the Center for Effective Medical Testing at ARUP Laboratories.

My eGFR was normal until I switched to a low-carb diet with intermittent fasting to control my blood glucose. That strategy worked well A1c dropped from 8 to 5.1 and has held 2 years. My creatinine has increased from 1.2 to 1.4. That small increase has alarmed my Doctor. I have read that ketosis causes increase in acetoacetate which interferes with the Jaffe method. Do you have any experience with low-carb diets?
I am not sure about your specific circumstance but a low carbohydrate diet can lead to the formation of ketone bodies. Ketone bodies are known to interfere with the Jaffee assay as described in this article:
Characterization of Creatinine Error in Ketotic Patients: A Prospective Comparison of Alkaline Picrate Methods with an Enzymatic Method
Stephen K. Gerard, M.D.. PH.D., H. Khayam-Bashi, PH.D.
American Journal of Clinical Pathology, Volume 84, Issue 5, 1 November 1985, Pages 659–664, https://doi.org/10.1093/ajcp/84.5.659
Published: 01 November 1985